Keratoconus Treatment in Calgary
What is Keratoconus?
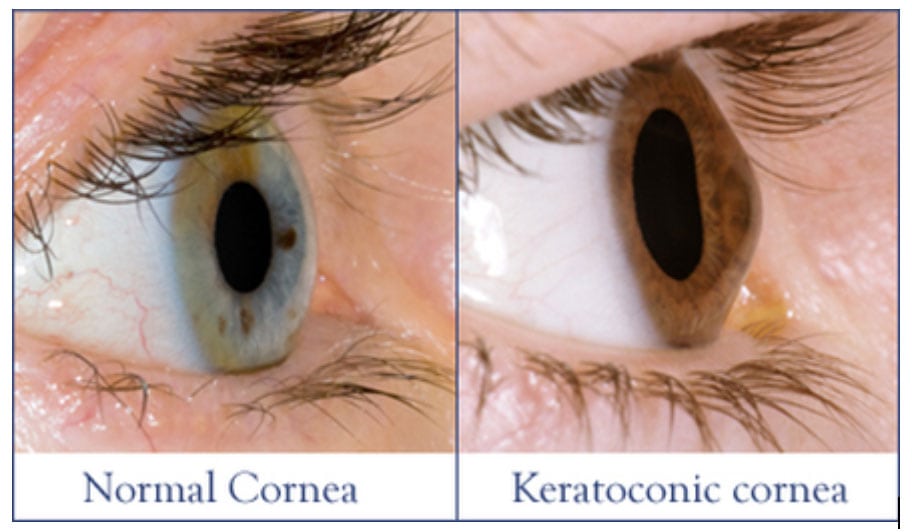
Keratoconus is a progressive thinning of the central cornea (the clear front window of the eye). This thinning weakens the structural integrity of the cornea causing it to protrude forward like a cone. Typically, keratoconus (KC) first presents at the age of puberty and progresses over the next 10-20 years. Eventually, after age 40-45, progression usually halts as the fibers of the cornea become more stiff with age. Severity of the disorder varies from very mild irregular astigmatism, to severe thinning, protrusion and eventually scarring.
Mission Eye Care is a leading provider in the diagnosis and management of keratoconus in Calgary and southern Alberta. We offer non-surgical optical correction for those with keratoconus. Our doctors have advanced residency training in specialty scleral and hybrid contact lens designs that can restore sharp vision.

How do I know if I have Keratoconus?
The prevalence of keratoconus is about 1 in 375 people. If we extrapolate that to the city of Calgary, with a population of 1.3 million people, there are expected to be about 4,000 people with KC within our city alone. The incidence (number of new cases per year) is 1 in 2000 people.
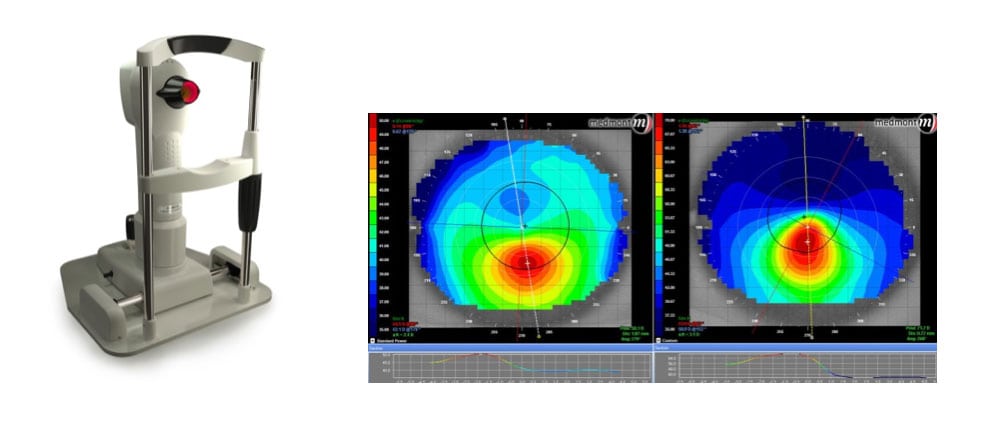
Patients with keratoconus often have mild astigmatism in the early stages. Over time, the astigmatism worsens, usually in one eye more than the other. This causes blurry vision, even while wearing glasses. Haloes and starbursts at night are also commonly noticed. At Mission Eye Care, we have advanced diagnostic equipment to detect keratoconus at an early stage. Testing includes topography, which measures the shape of the the cornea, and tomography, which measures the thickness of the cornea. Keratoconus typically shows up as steepening and thinning of the inferior cornea, resulting in blurry or distorted vision that does not fully improve with eyeglasses.
What causes Keratoconus?
The cause of keratoconus is still unknown. There are associations between keratoconus and atopy, Down’s syndrome, Leber’s congenital amaurosis, Ehler’s Danlos, and other connective tissue disorders. There does not appear to be a hereditary pattern, but it often does run in families. Keratoconus incidence has been found to be four times greater in Asian patients compared to Caucasian patients, and the disease also is generally more severe in the Asian population. Keratoconus is associated with a history of chronic, circular, eye-rubbing with the palms or knuckles. For this reason, refraining from eye rubbing is always recommended for patients with keratoconus.

What are treatments for Keratoconus?
If keratoconus is newly diagnosed in someone under the age of 40, it is most likely that a referral will be made for a procedure called Corneal Crosslinking (CXL), which stabilizes the corneal fibers to give them more rigidity and prevent further progression. CXL does not improve vision on its own, however, some surgeons elect to also perform a laser correction procedure at the same time as CXL to both halt progression of KC and reshape the cornea to improve vision.
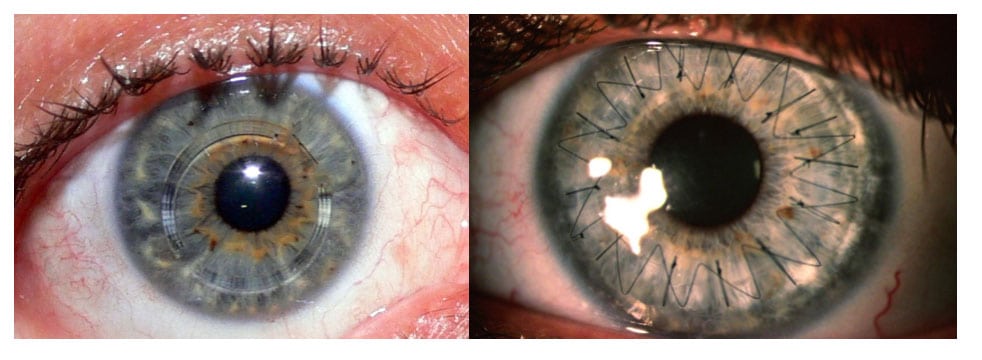
After CXL, vision usually corrects well with glasses or standard soft contact lenses, but in some cases, the corneal shape is still irregular. For these cases, specialty contact lenses have the potential to improve vision, in many cases, close to 20/20 vision can be regained with a properly fitted custom lens. These lenses are able to establish a spherical shape to the front of the eye, allowing light to focus properly onto the retina. At Mission Eye Care, our doctors have highly specialized and post graduate residency training in the fitting of these lenses. You can read more about these options here.
If the disease is advanced, if there is central corneal scarring, or thinning of the cornea to such an extent that rupturing may occur, then keratoplasty (corneal transplant) is recommended. This may involve a full-thickness transplant, or a partial transplant of only the anterior (front) layers of the cornea. Many patients will still require specialty contact lenses after transplantation.
Our clinic has long been one of the largest fitting centers for specialty contact lenses in Alberta. We invest in the latest tools and technology to provide world class care for our patients with keratoconus. Custom molded contact lenses can restore normal sight to those with keratoconus or those with corneal transplants. We are the only clinic in western Canada to have both the custom molded EyePrint prosthetic lenses and the BostonSight lenses for advanced corneal disease.